About Reiter’s Syndrome
A German army physician, Hans Reiter, first described this syndrome during World War I. Reiter described a disease with three features—an arthritis, a painful inflammation of the eye (conjunctivitis), and a discharge from the penis (urethritis) —in an army lieutenant. Later observers added a fourth feature sometimes characteristic of the disease, a particular skin rash called keratoderma blennorrhagica. Reiter’s syndrome is relatively rare compared to most of the forms of arthritis described in this article, but it is the second most common cause of arthritis in young men in their late teens or twenties. (Ankylosing spondylitis is the first.) Reiter’s syndrome is almost always a disease of men.
The same gene (B27) that is almost always present in ankylosing spondylitis is usually present in Reiter’s syndrome. Reiter’s patients have this gene from 70% to 90% of the time, compared with 7% in the general white population. (Like ankylosing spondylitis, Reiter’s syndrome is unusual among blacks.) Occasionally members of the same family may have the disease, underscoring the genetic effect, but family members are more likely to have ankylosing spondylitis than the rarer Reiter’s syndrome.

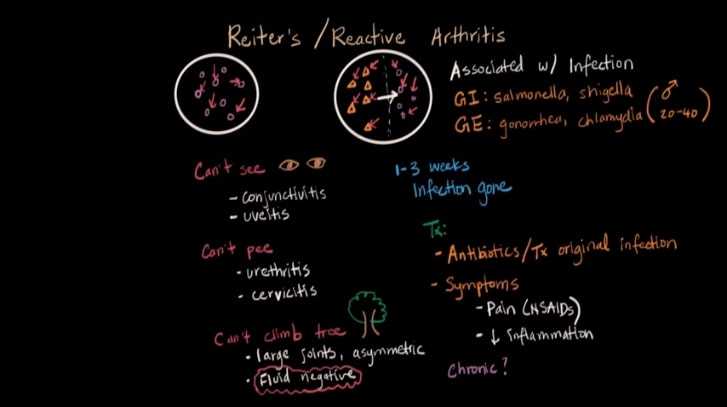
Infections seem to cause Reiter’s syndrome. The infection may occur several weeks before the development of the arthritis, the urethritis, and the conjunctivitis, and the infections seem to fall into two broad categories:
Those from venereal exposure and those related to diarrhea. In the United States there is usually a sexual exposure to the disease shortly before the development of discharge from the penis, which is usually the first symptom. Reiter’s syndrome is not considered a definite venereal disease, but most physicians think venereal exposure to be a likely cause in many cases. The infection appears to cause Reiter’s syndrome in those susceptible individuals with the B27 gene.
Another form of this syndrome follows episodes of diarrhea. This form can occur in epidemics and is most frequently related to shigella dysentery, a form of bacterial diarrhea. Several well-studied epidemics suggest that about 20% of subjects who are B27, positive and experience shigella dysentery will develop Reiter’s syndrome.
It seems likely that no single bacterium causes all cases. The Shigella infection is the best established, but some of the venereal cases appear to follow infection with organisms called Chlamydia or Mycoplasma. Somewhat similar problems are seen after infection with Yersinia or Salmonella organisms. Thus, different infectious syndromes may precede development of Reiter’s syndrome.
This interplay between the genetic predisposition represented by the B27 gene and the necessity for attack by a microorganism provides a fascinating interaction for scientific study. These studies, now being conducted at many medical centers, are likely to lead to major advances in managing Reiter’s syndrome.
Features of Reiter’s Syndrome
Reiter’s syndrome occurs mostly in men and is usually episodic, with each episode lasting several weeks to several months. It frequently recurs in subsequent years, and it shares many features with ankylosing spondylitis and psoriatic arthritis.
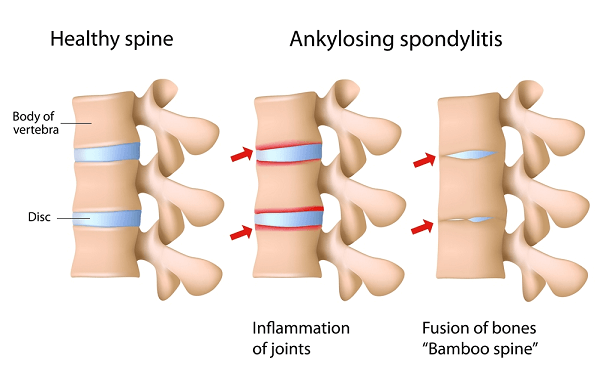

As with ankylosing spondylitis, the main problem is at the attachment where ligaments and tendons insert into the bone. Thus, involvement of the sacroiliac joints and of the spine is common. Since Reiter’s syndrome tends to involve the peripheral parts of the body more than ankylosing spondvlitis, a common feature is heel pain, either on the bottom of the heel where the ligaments that form the arch attach or on the back of the heel where the Achilles tendon attaches.

Like psoriatic arthritis, Reiter’s syndrome tends to involve the peripheral joints in a random way Thus, just a few joints are usually involved, and these joints are usually not the same on the two sides of the body. Reiter’s syndrome frequently involves one side of the body while sparing the other, and it may skip around from one side to the other in different parts of the spine. A “sausage digit,” as described on this article, is sometimes seen. In psoriatic arthritis, the upper extremities usually are involved more than the lower, while with Reiter’s syndrome the feet and toes are more frequently involved than are the hands.
Eye problems usually involve only one eye at a time. This may be conjunctivitis (“pink eye”) or an inflammation affecting the deeper parts of the eye, causing pain on exposure to bright light or interference with vision.
Discharge from the penis is the third major feature and usually consists of a clear, watery discharge that does not cause discomfort. While this frequently lasts only a few days or weeks, it may reappear later.
A skin rash occurs in only a few patients, but it can help with the diagnosis. The scaling red skin lesions are most common on the palms and soles and are sometimes not immediately noticed because they don’t hurt or itch. Shallow sores of the penis or of the female genital organs may occur; these are also usually painless. Some cases of Reiter’s syndrome with skin involvement resemble psoriatic arthritis, and distinction between the two can be difficult.
Tests
X-ray changes usually take several years to develop. Inflammation of the sacroiliac joint, as in ankylosing spondylitis, is common. Stiffening of the spine can also be seen. X-rays of the heels may show bone spurs at the points of attachment where the heel pain is noted.
Laboratory tests are not particularly helpful in diagnosis. The latex test for rheumatoid factor is negative. The antinuclear antibody test is negative. The sedimentation rate is sometimes elevated and sometimes not. The test for the B27 antigen will be positive about 70% of the time.

Prognosis
Reiter’s syndrome is characterized by an episodic course. Some patients have only one episode and no recurrences. For others, periods of activity of the disease will alternate with periods of relative inactivity. It is unusual for the arthritis to be severely crippling, but this can happen.
In a very few cases, problems with the eye can result in loss of sight, usually in just one eye and late in the disease. The skin problems seldom pose real difficulties and are usually present only a small part of the time.
Those individuals with Reiter’s syndrome who do not have the B27 gene probably do a little better than those who have the gene. The first episode usually gives some indication of the disease’s future severity. Like most forms of arthritis, Reiter’s syndrome varies from mild to severe, with most patients doing quite well.
Treatment
As in ankylosing spondylitis, the most frequent medications used are indomethacin and naproxen. In very severe cases, methotrexate , azathioprine, or experimental drugs may be required. Corticosteroids such as prednisone are not very helpful and should almost never be used.

Reiter’s syndrome is sometimes difficult to treat and may be resistant to all of the antiinflammatory agents. Sometimes a drug that seemed ineffective when first used will prove effective when used again a few weeks or even months later. Hence, when the disease is difficult to control the physician may periodically rotate drugs to determine which will work the best. Since the disease comes in cycles control can ultimately be achieved, but it may take disturbingly long to find the right treatment.
Although infections seem to cause Reiter’s syndrome antibiotics do not seem to be an effective treatment. Many physicians have tried tetracycline and other antibiotics, but the results have been inconsistent.
Eye involvement may require treatment with corticosteroids applied locally. In severe cases the steroid may be injected into the eye or behind the eye. The skin problems seldom require any treatment. Involvement of the aortic valve, exceedingly rare, may require replacement of that valve surgically.
Surgery for the joints is rarely needed in Reiter’s syndrome. Range-of-motion exercises and a judicious balance between rest and graded exercise are important.