Chronic Knee Pain Causes
Knee pain is one of the most common reasons people come to their primary care practitioner (PCP). 30% of all orthopedic complaints are related to knee pain. Over 50% of all athletes will complain of knee pain at some point in their lives.
Most people underestimate the seriousness of their chronic knee pain. By the time a person presents to their PCP they are often times past the point where preventive measures could have made a difference. So it is that the USA has the highest rate of knee replacement in the world.

This post will focus on chronic knee pain causes. My hope is that with early intervention, preventative treatments, and nutraceuticals, more joint replacements can be avoided.
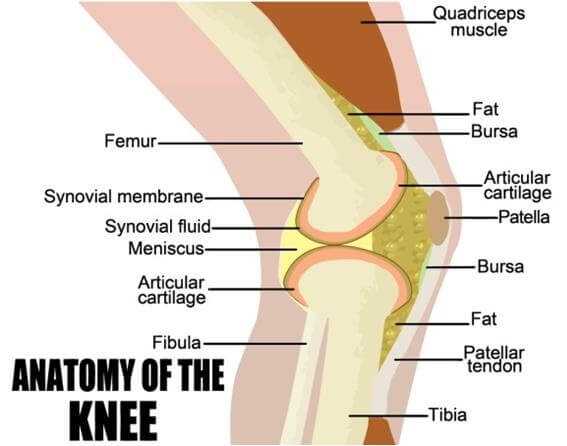
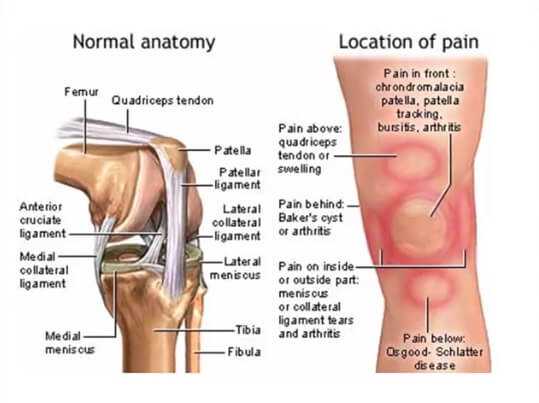
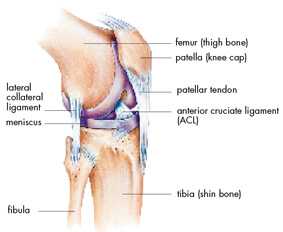
A Brief Review Of Knee Anatomy
The knee is a mechanically “at risk” joint. What I mean by that is that the very structure of the knee places mechanical forces on it that can amplify “wear and tear.”
You can think of the mechanical disadvantage of the knee this way…2 long poles attached by cords attempting to limit the backward and forward…side to side motion at the ends where the 2 poles meet…that’s the knee.
When the knee is involved in activity it moves in a multi-planar way (though its major motion is like a “swinging hinge”). In motion, all attachment and cartilage tissues of the knee are stressed. When standing erect the knee rotates slightly, “locks out,” and handles its weight load with a minimum of ligament and tendon strain.
The knee also has two curious interior structures called menisci (meniscus in the singular). The menisci guide the synovial surfaces of the knee and help decrease the “backward and forward – side to side” motion of the knee. They stabilize the sliding surfaces, disperse friction, and cushion the knee. They are made of fibro-cartilage (similar to the substance of the outer ring of a vertebral disc).
Even at bed rest the knee is moving (just ask a friend who has had knee surgery). There is no possible way to eliminate motion of the knee without fusing it. Fusion is a surgical procedure where the femur (upper leg bone) and tibia (lower leg bone) are surgically made into one long pole.
Although this may reduce or eliminate knee pain, the additional stress on other joints (namely the hip) often results in earlier hip dysfunction necessitating eventual surgery of the hip.
The knee is also the most commonly injured large joint of the body. Just watch an athletic contest where there is major body contact and you will see that there is at least one knee injury. It’s an “anatomical set-up” that the knee would get injured.
Even bracing of the knee gives it little support. Orthopedic studies done on football offensive lineman (the largest people in professional football) show that a knee brace works by reminding the lineman to reduce the strain on their knees by changing the way they block. It offers little measurable supportive help.
Given the anatomical disadvantage of the knee, just how does the knee work?
A Brief Review Of Knee Physiology
The knee is a “swinging-hinge” mechanism. The actual major motion is in the form of an arc. It is really an eccentric arc that places stress on different structures within the knee at different phases of its motion. The study of movement is called kinesiology.
In the standing position the knee ligaments (which attach one bone to another) and tendons (which attach muscle to bone) are at their least stress. The major stress standing is compressive and is applied to the cartilage located on the end of the tibia and femur (called synovial cartilage).
As the knee begins to bend, the patellar tendon begins to rise first (the patella is the “knee cap”). As motion continues, tension in most ligaments and tendons builds to reach maximum stress at the fully bent position (the “squat”). A full squat places the greatest tension on the majority of the structures of the knee.
Ironically, the knee is the most vulnerable to external forces in its least stressed position, the fully extended “locked” position (such as when standing straight upright). Presumably, this position allows external forces to separate the knee compartments easiest due to the ligaments and tendons not being taunt .
Ligament shearing remains a major mechanism of injury in sports. More recent orthopedic surgical techniques utilizing cadaver ligament and tendon transplants (called allograft transplants), as well as tendon transplants from one part of the body to another (called autograft transplants), have improved recovery from cruciate ligament tears.
Ligament looseness (called “laxity”), tendon looseness (also “laxity”), and loss of cartilage of the knee are usual with the aging process. Injury of the knee, at an earlier age, accelerates the aging process of it. If a human being lives long enough, especially one who has had an active athletic lifestyle, they will develop some category of knee problem.
Chronic knee pain is an inevitability for nearly all human beings of advanced age. In the next section I will discuss 3 common knee pain causes.
3 Common Knee Pain Causes
1) Osteoarthritis:
By far the most common cause for chronic knee pain is Osteoarthritis (OA). It is a process of loss of cartilage from the surface of the femur and tibia. Although partially genetically governed (some families develop this condition at an earlier age), the major mechanism for OA is progressive micro-trauma to the cartilage. This micro-trauma eventually outstrips the healing mechanism of the cartilage.

The cartilage then becomes less abundant and the cells that produce it decrease in number. Eventually pieces of cartilage are lost and “pitting” occurs. This “pitting” is akin to the potholes seen on the streets of major cities after a severe winter.
Exposed bone, local inflammation, ligamentous laxity, and reflex muscle fatigue (the body’s attempt to stabilize the knee) all contribute to the pain felt in OA of the knee. OA is the most common reason for total knee replacement.
2) Ligament Tears:
As I introduced previously, the knee is at a disadvantage structurally such that tears of ligaments, tendons, and the menisci are common. Ligaments sustain a tear according to the mechanism of the force that is applied.
Lateral and medial ligament tearing occurs when a high energy force is applied to the opposite side of the knee. Medial Collateral Ligament tears occur by a lateral force applied and vice versa.
Cruciate Ligament tears occur when the applied force is from the front or back of the knee. The Cruciate Ligaments (anterior and posterior) cross in the interior of the knee.
As the Anterior Cruciate ligament stabilizes the tibia from going too far anteriorly on the femur, a powerful force directed posteriorly against the femur (from the front) can tear this ligament. This usually occurs when the athlete themselves land or pivot awkwardly.
The Anterior Cruciate ligament accounts for 90% of the stability of the knee. It is a common injury in high velocity contact sports (such as in American style football). Recovery from this form of injury is difficult. Usually, an orthopedic surgical repair is needed with a tendon transplant.
Even with surgery, the full rehabilitation from an Anterior Cruciate ligament tear can be 1 or 2 years. The good news is that, post repair and rehab, the recovered function is quite good. Many professional athletes have recovered and returned to active status.
Chronic pain, after a partial tear of the Anterior Cruciate ligament, can occur if the resultant knee remains loose. The laxity causes excess motion which injures the menisci and synovial cartilage further. This is called Chronic ACL Deficiency.
3) Meniscal Tears:
As previously eluded to, the Menisci are 2 fibrocartilage discs that cushion and guide the surfaces of the tibia and femur. The injuries to the menisci occur when a severe shearing or compressive force is applied.
As the menisci age, the fibrocartilage becomes less flexible and sustains micro-trauma. As the blood supply to this structure is not robust, healing occurs slowly and is easily outpaced with repetitive micro-trauma.
Tearing of the menisci can occur horizontally, vertically, or on an angle. It can also be complete or incomplete. The result can be a unstable tear or a flap. Unstable tears or flaps require very slow and progressive rehabilitation. In many cases the removal of the involved meniscus is required for relief of pain.
The removal of a meniscus destabilizes a knee further which accelerates the development of Osteoarthritis of the knee. The decision to remove or not remove the meniscus is best advised by an experienced orthopedic surgeon.
Finally
I have reviewed the basic anatomy, physiology, and 3 major causes of chronic knee pain. This post has been intended to explain how chronic knee pain occurs. The 3 causes discussed do not constitute all the causes of chronic knee pain.
The treatment of chronic knee pain is very effective. I recommend you read my post on “Severe Chronic Arthritis” for a more in depth discussion of treatments for Osteoarthrits (click here for the link).
I would also recommend the following links for posts I have written related to this subject:
THIS POST IS NOT INTENDED AS A MEDICAL RECOMMENDATION. A THOROUGH EVALUATION BY A PRIMARY CARE PRACTITIONER IS RECOMMENDED BEFORE ANY MEDICAL DECISION SHOULD BE MADE. THIS POST IS INFORMATIONAL ONLY.
I hope you have enjoyed this post. If you have further questions please comment. I would love to hear from you and will respond to you promptly.
I wish you much joy and good health.
Facebook
Google+
Twitter
Pinterest
Reddit
Tumblr
Skype
StumbleUpon
WhatsApp
Email
Print
Telegram
Pocket
Delicious