Causes and Diagnosis of Scoliosis

In the case of the most common form of scoliosis, adolescent idiopathic scoliosis, there is not a clear causal agent and it is generally believed to be multi-factorial. Several causes have been implicated, but there is no consensus among scientists as to the cause of scoliosis.
The role of genetic factors in the development of this condition is general accepted. Scoliosis is most often diagnosed in women. In some cases, scoliosis exists at birth due to congenital vertebral anomalies. Sometimes the development of scoliosis during adolescence is due to an underlying abnormality such as a tethered spinal cord, but more often the cause is unknown or idiopathic, which has been inherited by many factors, including genetic.
The scoliosis often presents itself, or worsens during the adolescent growth spurt. In April 2017, researchers at Texas Scottish Rite Hospital for Children identified the first gene associated with idiopathic scoliosis, CHD7. The medical advance was the result of a study over 10 years and is described in the May 2017 issue of the American Journal of Human Genetics.
Risk Factors
Age: children from 4-6 weeks gestation at 3 years; Youths from 4 to 10 years of age, adolescents from 11 to 17 years.
Family members who have had scoliosis due to an inherited disease.
Delayed puberty and delayed menarche in girls.
Symptoms
Patients who have reached skeletal maturity are less likely to have a case of worsening. Some severe cases of scoliosis can lead to reduced lung capacity, putting pressure on the heart, and restriction of physical activities. The symptoms of scoliosis may include:
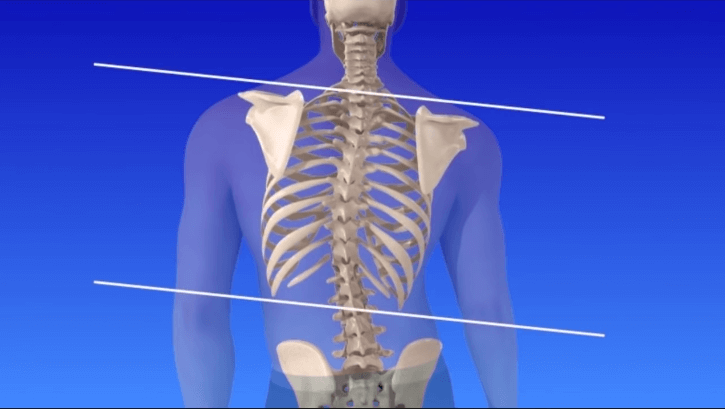
Uneven musculature on one side of the spine;
A rib importance and/or important scapula, caused by the rotation of the rib cage on thoracic scoliosis;
Uneven hips/leg length;
Asymmetric size or location of breast cancer in women;
Slow nerve action (in some cases).
Scoliosis Diagnosis
Patients who initially present with scoliosis are examined to determine if there is an underlying cause of the deformity.
During a physical examination, evaluate the following:
Skin spots are indicative of neurofibromatosis;
The feet of the deformity cavovarus;
Abdominal reflexes;
Muscle tone for spasticity.
During the examination, the patient is asked to remove their shirt and lean forward. (This is known as the forward-bending Adams test and is often performed by students of the school). If you see a prominence, then scoliosis is a possibility and the patient should be sent to an X-ray for diagnosis.

Alternatively, a scoliometer can be used to diagnose the disease. The patient’s gait is assessed, and a test for signs of other abnormalities (e.g. spina bifida as evidenced by a dimple, hairy, lipoma or hemangioma).

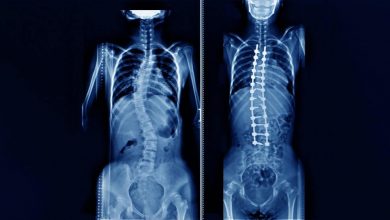
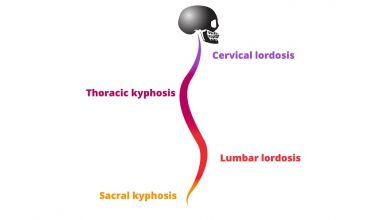
A complete neurological examination can be done as well. It is usual when scoliosis is suspected, that they have a full weight-bearing spine AP/coronal (frontal posterior view) and lateral/sagittal (side view) X-ray taken to evaluate the curves scoliosis, kyphosis and lordosis, as these may also be affected in people with scoliosis.
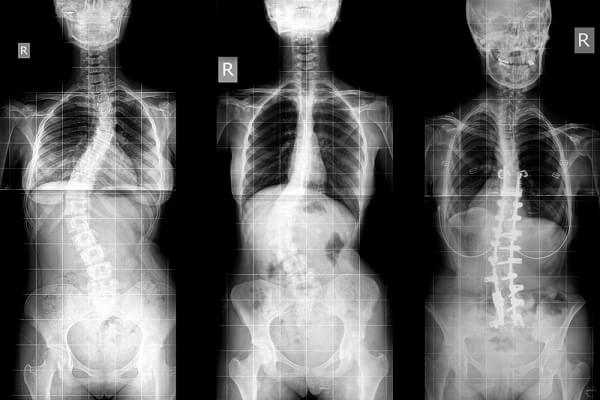
Full-length standing spine X rays are the standard method for assessing the severity and progression of scoliosis, and whether it is congenital or idiopathic in nature. In growing individuals, serial radiographs are obtained at intervals of 3-12 months and follow the progression of the curve. In some instances, MRI investigation is warranted to examine the spinal cord.
The standard method to quantitatively assess the curve is the Cobb angle measurement. The Cobb angle is the angle between two lines, perpendicular to the superior endplate of the upper vertebra and the inferior endplate involving the lower vertebrae that is affected.
For patients who have two curves, Cobb angles are followed for the two curves. In some patients, lateral bending x-rays are obtained to assess the flexibility of the curves or the curves of primary and compensation. Genetic testing for AIS, which is available in 2009 and is still under investigation, attempts to measure the risk of progression of the curve.
Scoliosis Management
The traditional medical treatment of scoliosis is complex and is determined by the severity of the curvature and skeletal maturity, which together help predict the likelihood of progression.
The conventional options are, in order:
Observation;
Physiotherapy;
Bracing;
Surgery.
A growing body of scientific research demonstrates the effectiveness of specialized treatment programs of physical therapy. The debate in the scientific community about whether chiropractic and physical therapy can influence the curvature of scoliosis is partly complicated by the variety of proposed methods and employees: some are supported by more research than others.
Methods of physiotherapy
The Schroth method is a non-invasive physical therapy treatment for scoliosis that has been used successfully in Europe since the early 1920s. Originally developed in Germany by a victim of scoliosis Katharina Schroth, this method is taught to patients in clinics specifically devoted to Schroth scoliosis treatment in Germany, Spain, England and more recently, the United States.
The method is based on the concept of scoliosis as a result of a complex of muscle imbalances (especially the power imbalances in the back) that can be at least partially corrected by exercise). Small curvatures between 15 and 20 ° during growth can be treated with the physio-logic of the program and between 5 and 20, a 30 ° spurt with “3D-Made-Easy.”
This program has been tested in the environment of hospital treatment and in the curves above 30° a combination of these methods, along with the Schroth program can be useful.
This is important
A specialized center with trained and certified personnel must be taken into account. As for the rehabilitation treatment of patients today one can achieve the same result as in the programs of the patients. Also, outside patient programs can succeed if given the specific pattern programs.
A certain intensity is certainly necessary to enable better compliance with conservative treatment in order to acquire coping strategies to enable one to live with the deformity and with conservative treatment.
The indications for treatment are dependant on the size of the curve, the maturity of the patient and the individual curve pattern. However current conservative management of scoliosis can be regarded as evidence based, while there is not enough long term data available for the treatment.
For more information about scoliosis, click “All About Scoliosis“.