Options For Chronic Pain And Addiction

Chronic pain and addiction remains one of the most controversial areas in medicine today. There is still a misunderstood belief that the use of prescription pain medication for chronic pain (particularly opioid pain medications) will “make” a person an addict. In fact, this is the premise for the restrictive guidelines recently put forth by the Centers for Disease Control
This is still stubbornly believed by patients and Doctors alike. The incidence of denovo opiate addiction in the United States is 3% – 16 %…a statistic that has not changed since the Civil War.
Furthermore, good research in the area of opiate abuse is lacking. Most of the existing studies were poorly structured and did not follow strict empiric scientific method. The bias of the sponsor of these studies is usually quite obvious.
Also, what is to be done about people who have been addicts and have chronic pain? Are they disqualified from prescription pain medicine? Are people who are alcoholics, mentally unstable, or use marijuana also disqualified?
In today’s predatory prosecution of pain management physicians, these issues have not been addressed with good placebo controlled prospective studies. In addition, the fear of legal reprisal demotivates Doctors who are already ambivalent about chronic pain medications.
The History As A Guide To The Risk Of Addiction
Unfortunately, the history alone is unreliable as an indicator of how a person will do on chronic pain medication. No psychological, neurological, or sociological history can reliably predict whether a person with chronic pain will become addicted to chronic pain medications (other than already being an addict).
The best way to tell whether a person is having addictive complications is to follow them while taking their medications. Even then, openess and honesty in the Doctor – Patient relationship is essential as the Doctor is not a prophet.
Not treating chronic pain has inherent risks (early death from suicide, heart attack, stroke, etc.). There is no “risk free” option in chronic pain management.
The Physical Exam As A Guide To The Risk Of Addiction
The ethnic background, appearance, number of tattoos, muscularity, beard configuration, etc. have all been shown to not correlate with whether a person becomes addicted to their prescription pain medications or not.
There has never been any physical finding that predicts whether a person on chronic pain medication will become addicted. The many biases in this area have never been proven by scientific studies.
The Best Way To Predict Addiction Is Close Follow-Up
So what is the Doctor, who wants to show compassion and treat his patient, to do? I am going to suggest the following sensible guidelines:
- First prove that the person has been correctly diagnosed with a disorder that would cause chronic pain. This will usually have required a “work-up” that included a thorough History and Physical, Diagnostic studies, and often a subspecialist’s consultation.
- An assessment of the psychological state of the hurting patient.
- A narcotic contract be presented to the person that outlines expectations for the relationship between the treating Doctor and the patient. It will usually require regular urine drug screening, regular visits, and a single physician to prescribe the pain medications.
- The pain level of the patient should be documented at each visit (the “1 -10” pain scale is the standard).
- The patient should be given an opportunity for a “test period” to see how they handle the medications (usually 2 weeks to 1 month).
- A reassessment should be done shortly after the test period begins.
- Openness and honesty, on the part of the patient and their family, is essential for correct assessment of their response to the medications.
And Finally
It is not more righteous to leave a patient in pain to avoid addiction. There must be more grace in how we approach the “brain disease” called addiction. Is it not curious that, despite the “war on drugs”, the incidence of drug addiction has not changed since 1865?
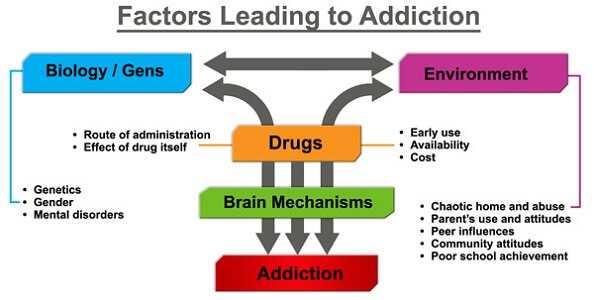
The use of opiates as the major risk factor for addiction is a simplistic approach to addiction. Addiction is a complicated disorder that requires an understanding of the genetic, physiological, social, and emotional issues that may lead to addiction. Dr. Carl Hart of Columbia University calls this the “cage we live in.” It depends on the “cage we live in” whether addiction develops or not when taking opiates.
In medicine, the Doctors creed had always been…”Cure occasionally…Treat most…and comfort always”. Is it possible we could return to this as our “prime directive”?
If you have a question or comment please enter it below. I would love to be of service to you.
Wishing you joy and healing.
Facebook
Google+
Twitter
Pinterest
Reddit
Tumblr
StumbleUpon