Rheumatoid Arthritis Surgery Options
Synovial Facet Joint Removal for Rheumatoid Arthritis
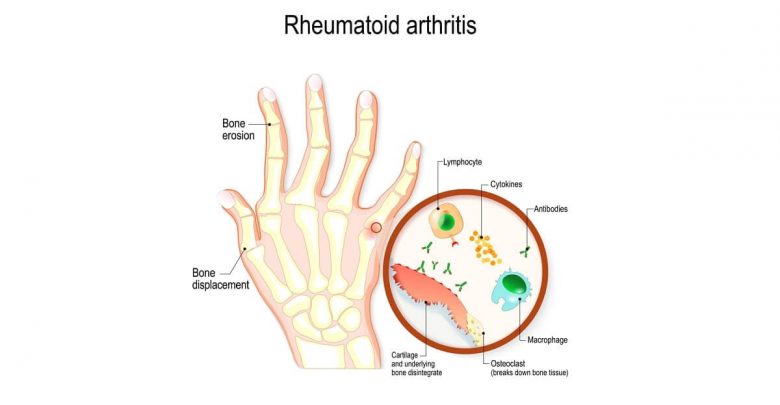
As Rheumatoid Arthritis is an inflammatory condition where the body’s own immune system attacks tissues including the synovial membranes around the joints, the lubrication between facet joints in the spine can be eroded. This leads to the bones rubbing together and causing pain and instability. The growth of osteophytes is the body’s way of trying to re-establish that stability but can cause pinched nerves and cord compression. If the facet joints become hypertrophic then they may need removing or parts may need to be excised in order to decompress the spine. The body’s immune system may also attack cartilage and bone, which can then cause further problems and may not be efficiently addressed through back surgery using bone grafts taken from the patient themselves.
Laminectomy, Laminotomy, and Laminoplasty for Rheumatoid Arthritis
Laminectomy is a back surgery done to remove a section of the thickened ligament covering the spinal canal in order to allow more space for the spinal cord and spinal nerves to relax into. It is often followed by fusion in order to restore the stability of the spine that may be lost after removing this major structural element of the spinal column. Surgery is invasive and can take many weeks, if not months, to recover from. For many patients with Rheumatoid Arthritis the potential benefits of such surgery do not compensate for the extra disability and pain during the recovery period.
A slightly less invasive surgery is a laminotomy, where a small window is cut into the lamina to allow the spinal cord to relax into the newly created space. As less of the lamina is excised in this procedure the patient may not need spinal fusion. Unfortunately, the level of decompression achieved by this type of surgery is often difficult to judge during the surgery making the risk of failed back surgery a little higher. Techniques to improve the procedure have included the use of a fluoroscope to assess the level of decompression, and the combination of the operation with a foraminotomy in a microlaminoforaminotomy procedure.
A laminoplasty does not involve the removal of the lamina but does significantly affect the structure of the back bone by cutting one side in order to create a hinged effect. This hinged lamina is held in place using metal instrumentation and creates more space for the spinal nerves and spinal cord to decompress. The stability of the spine may be better maintained than in a laminectomy, and the level of decompression achievable using this approach is often better than for a laminotomy. Patients with Rheumatoid Arthritis may not be able to achieve significant benefits from these more minimally invasive surgeries however, as the degree of osteophyte growth or structural defect may require more extensive tissue removal.
Foraminotomy and Corpectomy for Rheumatoid Arthritis
A foraminotomy is a back surgery designed to increase the available space for the nerves as they exit the spine through small gaps called foramina. These foramina can become obstructed by the growth of osteophytes, herniated, bulging, or ruptured disc material, and by structural defects. Major structural problems are not addressed by this procedure, however, and it is often only helpful for patients with a fairly early stage of Rheumatoid Arthritis. Compression on the spinal cord will not be relieved using this procedure, however, and so a separate operation such as a laminotomy, laminoplasty, or laminectomy, may also be required.
Rheumatoid Arthritis patients may undergo a corpectomy, also known as a vertebrectomy, where the surgeon removes a part, or the whole, of a vertebral body due to significant osteophyte growth which is causing a pinched nerve or spinal cord compression. The surgeon can also remove the intervertebral disc if this is contributing to the compression. The spine will be unstable after such a procedure, in most patients, and requires fusion to avoid future spinal slippage (spondylolisthesis).