The Phantom Of Pain

No one grows up thinking they will have a body part removed during their lifetime. Every year 185,000 people in the US have an amputation of one sort or another.
Afterwards, many will be visited by a “phantom” and that “phantom” called “Phantom Pain” will be their companion for life. This blog will discuss the enigma of Phantom Pain…pain described to be in the region of an amputated body part.
Most Phantom Pain (PP) occurs in people that have lost a limb. One in every two hundred Americans will have an amputation. The most common causes are vascular compromise (often due to Diabetes Mellitus) in 54% and trauma in 45%.
However, PP does not just occur in amputations. Women who have had a Mastectomy, men who have had a Prostatectomy, people with teeth extracted, and even those that have lost an eye may all suffer from PP. Essentially any body part that has been removed can be a “set-up” for PP.
People who have PP are often reluctant to disclose it. They sound a bit crazy and realize it. Many are referred for Psychiatric consultation by their Primary Care Practitioner.
Fortunately, most amputees do not end up with chronic PP. While 60-80% of amputees have phantom sensations shortly after the amputation, most will resolve within 6 months. The unfortunate few that continue to have PP beyond 6 months often have the syndrome for the rest of their life.
How Does “Phantom Pain” Feel?
The amputee then, has to not only cope with the physical, emotional, and financial effects of their malady, but with PP too. The sensations in PP are not imaginary. PP reveals just how complex and individualized the sensation of pain can be.
Some people feel a tightness or squeezing. If their hand is amputated they may describe the sensation as a tightly clenched fist on the amputated side! Tingling, heat, and cold are also described. Nearly any sensation that could be detected before the amputation may be experienced in the amputated body region in PP. And the pain in PP is not consistent. The same area can have different types of PP at different times.
The general rule is that the discomfort can be provoked by many different factors. Stress, anxiety, changes in weather, sexual activity, light touch, smoking, urination, and even defecation may all provoke the discomfort. The provocation occurs despite the stimulus being quite remote to the amputated body part.
Why Does It Happen?
The exact physiologic reason that PP occurs is still uncertain. It appears to be an interaction between the severed nerve fibers of the amputated body part and the pain processing area in the brain associated with that body part.
Sometimes the severed nerves are able to generate pain impulses on their own. They may, in fact, be over-sensitive once they have healed. This “auto-generator” then interacts with the sensory portion of the brain normally connected to the amputated body part.
The brain needs regular input of information to function normally. When an amputation occurs the usual information from that body area is lacking. The associated brain connection becomes “starved” for information and eventually “reassigns” the brain region with a new body part. For reasons not yet explainable, the reassignment of the brain map (previously attached to the amputated part) causes PP.
Sometimes the reassignment enhances another body part function. So it is that blindness can result in exquisite hearing (consider Stevie Wonder or Ray Charles). Also consider the exquisite sense of touch the deaf may have (do you remember Helen Keller).
The tendency to develop PP is higher in people who had a long period of time where the amputated part was malfunctioning before amputation. It is almost like a neurologic “wind-up” occurs. It would seem that the “wind-up” sets-up the reassignment to be interpreted as PP.
Also, severe traumatic amputations (such as in war) have a higher likelihood of PP. This may be due to emotional “wind-up” related to warfare.
How Do I Treat It?
Up until recently, treatment was fairly ineffective. But, with the advances in our understanding through Neuroscience, a number of very promising therapies have been developed. Here are a few:
- Biofeedback: Adaptive control of autonomic functions through learning.
- Medications: Anti-depressants, Opiates, Anti-epileptics, and some natural remedies.
- Acupuncture: Effects neuro-transmission by cutaneous reflexes.
- Massage Therapy: similar to acupuncture.
- Hypnosis: blocks central pain mediation through ” willful disattention.”
- Relaxation Training: causes the release of endorphines (pain reducing chemicals in the brain).
- Physical Therapy: as per relaxation training.
- Vibration Therapy: as per relaxation training.
- Transcutaneous Electrical Nerve Stimulation: similar mechanism to acupuncture.
- Local Injections of the stump: reduces severed nerve irritatbility in the amputated body part.
- Spinal Nerve Blocks: reduces nerve transmission for pain perception.
- Sympathetic Nerve Blocks: as per spinal blocks.
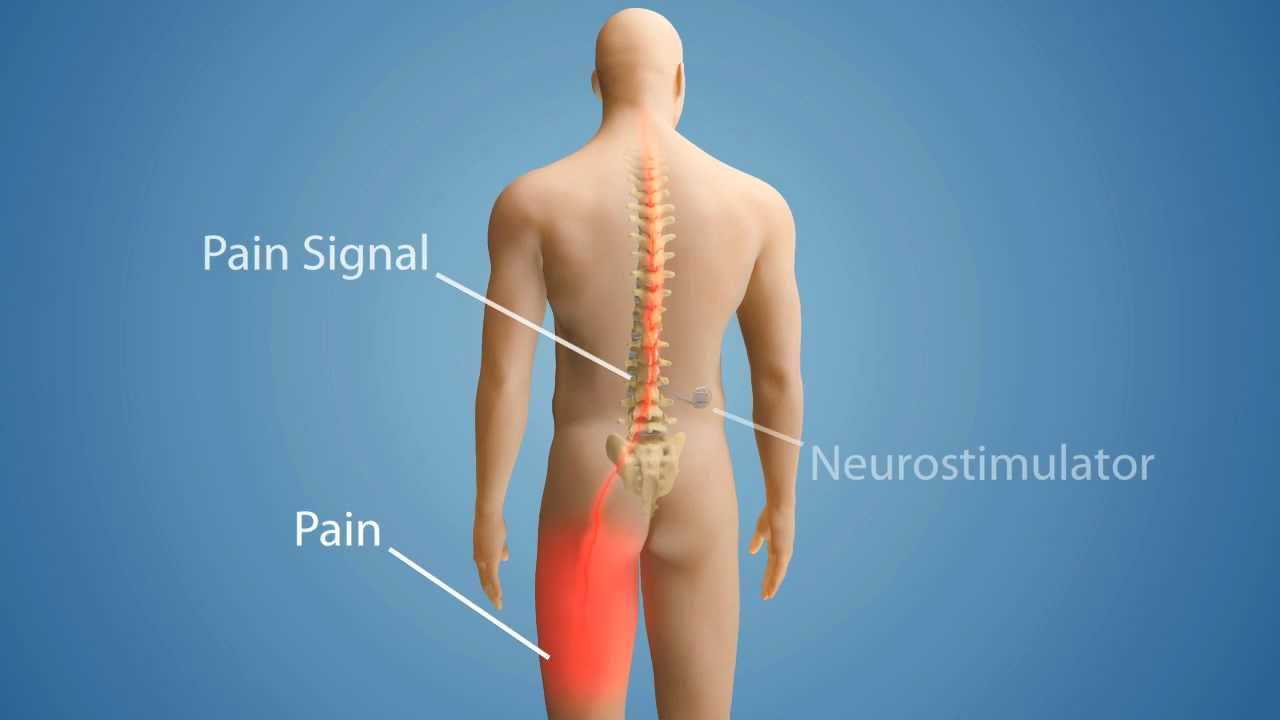
- Spinal Cord and Brain Deep Stimulation: mixed mechanisms of action in the spinal cord and brain.
“Mirror Box” Therapy: See the digital video below. This is one of the most effective forms of treatment for PP:
Finally
I have discussed Phantom Pain, how it feels, how it happens, and how to treat it. There is new hope for people suffering with this malady. As our understanding of Neuroscience grows I can only believe that our therapies for PP will improve. The present interest in this malady is at an all time high since there are such a large number of our wounded veterans returning with it from the Middle East.
Wishing you joy and healing.
I would also like to hear from you. Please leave a comment or question below. I will promptly return your message.